
Description: The American Diabetes Association (ADA) updates the Standards of Medical Care in Diabetes annually to provide clinicians, patients, researchers, payers, and other interested parties with evidence-based recommendations for the diagnosis and management of diabetes.
Methods: To develop the 2020 Standards, the ADA Professional Practice Committee, comprising physicians, adult and pe-
diatric endocrinologists, diabetes educators, registered dietitians, epidemiologists, pharmacists, and public health experts, continuously searched MEDLINE (English language only) from 15 October 2018 through August–September 2019 for pertinent studies, including high-quality trials that addressed pharmacologic management of type 2 diabetes. The committee selected and reviewed the studies, developed the recommendations, and solicited feedback from the larger clinical community.
Recommendations: This synopsis focuses on guidance relating to the pharmacologic treatment of adults with type 2 diabetes. Recommendations address oral and noninsulin injectable therapies, insulin treatment, and combination injectable therapies. Results of recent large trials with cardiovascular and renal outcomes are emphasized.
In 2020, the American Diabetes Association (ADA) made important additions to the section on pharmacologic approaches to glycemic treatment of type 2 diabetes in the Standards of Medical Care in Diabetes. On the basis of new evidence, the ADA added a recommendation on early combination therapy for type 2 diabetes to extend the time to treatment failure. It is now recommended that these drugs be considered for patients in whom atherosclerotic cardiovascular disease (ASCVD), heart failure, or chronic kidney disease (CKD) predominate. The full position statement on pharmacologic treatment can be accessed at care.diabetesjournals.org/content/43/Supplement_1/S98. This synopsis summarizes the recommendations related to pharmacologic management and highlights important evidence from recent large trials with cardiovascular and renal outcomes.
GUIDELINE DEVELOPMENT AND EVIDENCE GRADING
The Professional Practice Committee of the ADA is an expert committee that comprises physicians, diabetes educators, and others who have expertise in such areas as pediatric and adult endocrinology, epidemiology, public health, microvascular complications, cardiovascular risk management, preconception and pregnancy care, diabetes prevention and weight management, and the use of technology in diabetes. For the current revision, committee members systematically searched MEDLINE for pertinent studies published in English from 15 October 2018 to August–September 2019. Committee members reviewed selected studies and, on the basis of new evidence and as needed, revised recommendations, clarified previous recommendations, or aligned the strength of the wording to the evidence.
Recommendations are rated A (well-designed clinical trials or high-quality meta-analyses), B (well-conducted cohort studies), C (uncontrolled studies), or E (expert consensus or clinical experience). The ADA funds development of the Standards of Care from its general revenues, with no industry involvement or support. Detailed information about the committee members and their conflict-of-interest disclosures, methodology, and the complete Standards of Care can be downloaded at professional.diabetes.org/soc.
PHARMACOLOGIC THERAPY FOR TYPE 2
DIABETES: RECOMMENDATIONS
Metformin is the preferred initial pharmacologic agent for the treatment of type 2 diabetes (Grade A recommendation).
Early combination therapy can be considered in some patients at treatment initiation to extend the time to treatment failure (Grade A recommendation).
The early introduction of insulin should be considered if there is evidence of ongoing catabolism (weight loss), if symptoms of hyperglycemia are present, or when hemoglobin A1c (HbA1c) or blood glucose levels are very high (HbA1c >10% [86 mmol/mol], blood glucose ≥16.7mmol/L [300 mg/dL]) (Grade E recommendation).
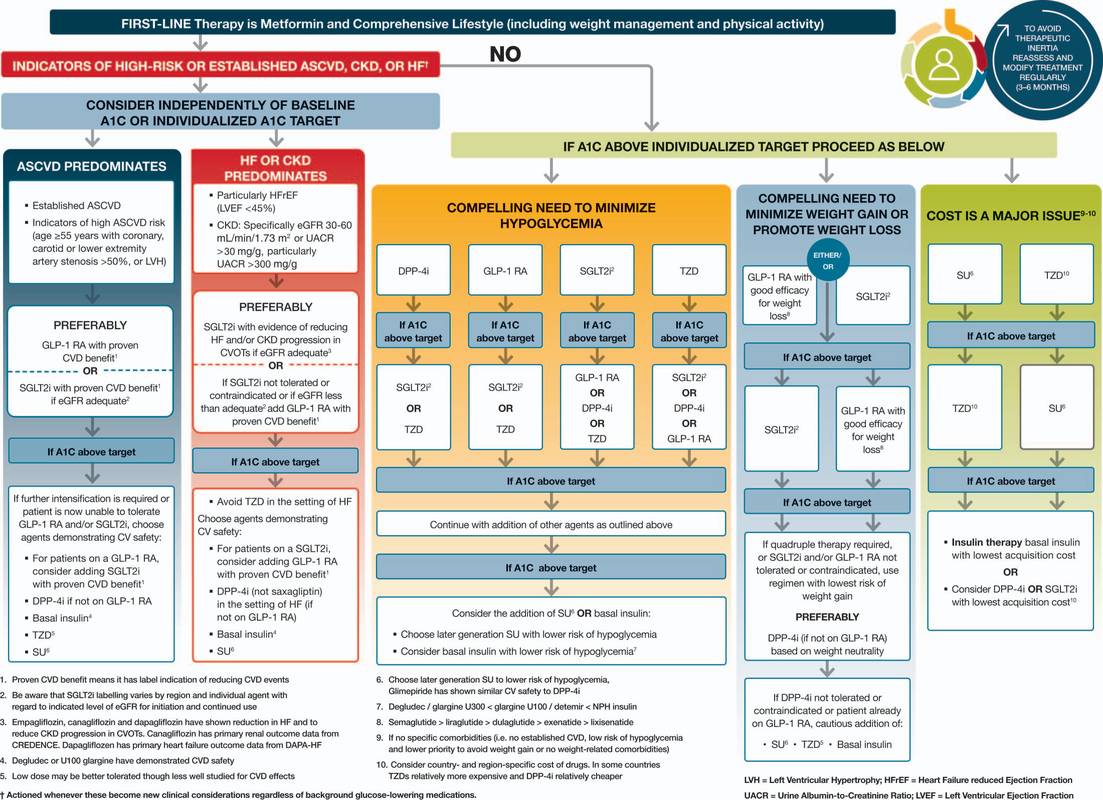
A patient-centered approach should be used to guide the choice of pharmacologic agents. Considerations include cardiovascular comorbid conditions, hypoglycemia risk, impact on weight, cost, risk for side effects, and patient preferences (Appendix Figure [available at Annals.org] and Figure 1) (Grade E recommendation).
Among patients with type 2 diabetes who have established ASCVD or indicators of high risk, established kidney disease, or heart failure, a sodium–glucose cotransporter-2 (SGLT2) inhibitor or glucagon-like peptide-1 receptoragonist (GLP-1 RA) with demonstrated cardiovascular disease benefit is recommended (Grade A recommendation).
In patients with type 2 diabetes who need greater glucose lowering than can be obtained with oral agents, GLP-1 RAs are preferred to insulin when possible (Grade B recommendation).
The medication regimen and medication-taking behavior should be reevaluated at regular intervals (every 3 to 6 months) and adjusted as needed to incorporate specific factors that affect choice of treatment (Grade E recommendation).
INITIAL THERAPY
The mainstay for initial treatment of type 2 diabetes includes therapeutic lifestyle change. In addition, metformin is recommended as the initial pharmacotherapyin most patients with type 2 diabetes at the time of diagnosis. Metformin is considered safe and effective (1% to 1.5% reduction in HbA1c levels) in patients with no contraindications (such as stage 4 or 5 CKD, advanced heart failure, or a history of lactic acidosis). It may reduce the risk for cardiovascular events and death in persons who are overweight or obese (1). In some patients, it causes substantial gastrointestinal side effects, including bloating, abdominal pain, and diarrhea. For those who do not tolerate the medication because of gastrointestinal side effects, the extended release formulation may be more acceptable. Long-term metformin use has been associated with vitamin B12 deficiency and worsening neuropathy (2). Periodic testing of vitamin B12 levels may be reasonable (3). The U.S. Food and Drug Administration (FDA) recommends that metformin be used only in patients with an estimated glomerular filtration rate of 30 mL/min/1.73 m2 or greater (4). For patients who do not tolerate metformin or have contraindications to its use, alternative pharmacotherapy should be considered.
COMBINATION THERAPY
For patients who have symptoms from advanced hyperglycemia, insulin therapy is recommended to reduce glucotoxicity and lipotoxicity. It is common practice to initiate insulin therapy for patients who presentwith the following: a blood glucose level of 16.7 mmol/L (300 mg/dL) or greater or an HbA1c concentration higher than 10% (86 mmol/mol), symptoms of hyperglycemia (namely polyuria or polydipsia), or evidence of catabolic weight loss or ketosis (Figure 2). As glucose toxicity resolves, simplifying the treatment regimen or transitioning to oral agents is often possible.
Type 2 diabetes is a progressive disease, and combination therapy is often needed to achieve or maintain glycemic targets (a comprehensive discussion on glycemic targets can be found at care.diabetesjournals.org/content/43/Supplement_1/S66). Current recommendations advise a stepwise approach to treatment for most patients, with the sequential addition of other medications to metformin therapy if the HbA1c target is not achieved after approximately 3 months. Initial combination therapy should be considered in patients presenting with HbA1c levels 1.5% to 2% above target, because most medications rarely decrease HbA1c concentrations by more than 1%. Data exist to support initial combination therapy (5, 6). This approach may be superior to sequential addition of medications for both achieving glycemic goals more rapidly and maintaining glycemic control for a longer period (7).
Second-line medication options include SGLT2 inhibitors, GLP-1 RAs, dipeptidyl peptidase-4 (DPP-4) inhibitors, thiazolidinedione, sulfonylureas, and basal insulin. Clinical evidence suggests that each new non-insulin medication added to metformin generally lowers HbA1c levels by approximately 0.7% to 1.0% (8, 9). The choice of agent to add to metformin therapy should be individualized on the basis of patient characteristics, preferences, and drug-specific effects. Important patient characteristics include ASCVD, risk for ASCVD, heart failure, CKD, other comorbid conditions, and the propensity for specific medication-related adverse effects. Medication considerations include efficacy, safety, tolerability, ease of use, and cost.
The first step in deciding which medication should be added to metformin is to determine whether the patient has established ASCVD or a high ASCVD risk (patients aged ≥55 years with coronary, carotid, or lower-extremity artery stenosis >50% or left ventricular hypertrophy), heart failure, or established CKD. If the patient has 1 of these characteristics, an SGLT2 inhibitor or GLP-1 RA with demonstrated CVD benefit is recommended. The addition of these medications should be considered independent from HbA1c level in this patient population. If a patient has heart failure or CKD, an SGLT2 inhibitor is recommended. If an SGLT2 inhibitor cannot be used, a GLP-1 RA should be administered. For patients without established ASCVD, indicators of high ASCVD risk, CKD, or heart failure, the choice of a second agent is based on avoidance of side effects, particularly hypoglycemia and weight gain; cost; and patient preferences (10). If the main patient factor is cost, a sulfonylurea or thiazolidinedione should be considered. These medications are inexpensive and potent. If the main concern is avoiding hypoglycemia, preferred medications include GLP-1 RAs, SGLT2 inhibitors, DPP-4 inhibitors, or a thiazolidinedione. If a compelling need exists to minimize weight gain or promote weight loss, the preferred pharmacotherapy should include GLP-1 RAs or SGLT2 inhibitors. Metformin and DPP-4 inhibitors tend to be weight neutral. Similar considerations apply to patients requiring a third agent to achieve glycemic goals. Treatment regimens should be reviewed continuously for side effects, efficacy, and treatment burden. Some patients may need their medication reduced or withdrawn. Common reasons include intolerable side effects, drug ineffectiveness, drug costs, or a change in glycemic targets. In older adults, relaxing glycemic targets and de-escalating therapy are often appropriate steps, depending on the patient’s health status.
Although many patients prefer oral medications, injectable agents often are needed to achieve treatment goals. The 2020 Standards of Care state that if injectable therapy is needed to reduce HbA1c levels, then a GLP-1 RA should be considered in most patients before the use of insulin. Most GLP-1 RAs are injected, although an oral formulation of semaglutide is now available (11). Meta-analyses comparing injectable GLP-1 RAs with insulin in patients needing further glucose lowering indicate similar efficacy between the 2 treatments (12–14). In addition, GLP-1 RAs have the benefit of causing weight loss, rather than weight gain, compared with insulin and carry a lower risk for hypoglycemia.
The cost of diabetes drugs has increased substantially during the past 2 decades (15). Diabetes drug prices may be a major source of stress for patients and contribute to reduced adherence (16). Cost-containing strategies may improve medication taking behaviors in some patients (17).

CARDIOVASCULAR AND RENAL OUTCOMES TRIALS
Because of concerns that diabetes drugs might lower glucose levels but lead to adverse cardiovascular outcomes, the FDA issued guidance for industry in 2008 requiring large long-term cardiovascular outcome trials of all new medications for treating type 2 diabetes (18). In such outcome trials of DPP-4 inhibitors, SGLT2 inhibitors, and GLP-1 RAs, the study drug is compared with placebo, with both agents given in addition to standard care.
DPP-4 Inhibitor Trials
Trials of DPP-4 inhibitors met the primary outcome of noninferiority, meaning the studies demonstrated that DPP-4 inhibitors do not increase adverse cardiovascular outcomes. However, DPP-4 inhibitors have not demonstrated superiority, meaning that they have not shown cardiovascular benefits relative to placebo.
SGLT2 Inhibitor Trials
EMPA-REG OUTCOME (Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients Removing Excess Glucose) showed that empagliflozin reduced the risk for major adverse cardiovascular events (a composite outcome of myocardial infarction, stroke, and cardiovascular death), cardiovascular death, and hospitalization for heart failure (19). These results led to an FDA indication for empagliflozin for reducing the risk for cardiovascular death in adults with type 2 diabetes and cardiovascular disease. A prespecified secondary analysis of the trial showed that empagliflozin also reduced the risk for incident or worsening nephropathy (20).
Canagliflozin reduced the risk for major adverse cardiovascular events but increased the risk for fracture and lower-limb amputation in CANVAS (Canagliflozin Cardiovascular Assessment Study) (21). The CREDENCE (Canagliflozin and Renal Events in Diabetes With Established Nephropathy Clinical Evaluation) trial involved patients with chronic diabetes-related kidney disease, most (99%) of whom were using an angiotensin-converting enzyme inhibitor or angiotensin-receptor blocker (21). In this trial, canagliflozin reduced the risk for worsening kidney disease and death (a composite outcome of end-stage kidney disease, doubling of serum creatinine levels, or death from renal or cardiovascular causes), major adverse cardiovascular events, and hospitalizations for heart failure. Canagliflozin did not statistically significantly increase the risk for lower-limb amputations, fractures, acute kidney in- jury, or hyperkalemia but did increase the risk for diabetic ketoacidosis (2.2 and 0.2 events per 1000 patient-years in the canagliflozin and placebo groups, respectively). In September 2019, the FDA approved canagliflozin to reduce the risk for end-stage kidney disease, doubling of serum creatinine levels, cardiovascular death, and hospitalization for heart failure in adults with type 2 diabetes and diabetic nephropathy with albuminuria greater than 300 mg/g.
In the DECLARE-TIMI 58 (Dapagliflozin Effect on Cardiovascular Events–Thrombolysis in Myocardial Infarction 58) trial, dapagliflozin met the prespecified criteria for noninferiority to placebo with regard to major adverse cardiovascular events, but superiority to placebo was not demonstrated (22). Dapagliflozin reduced the risk for a coprimary composite end point of cardiovascular death or hospitalization for heart failure, driven primarily by the hospitalization end point. No between-group differences were demonstrated for cardiovascular death, rate of amputation, fracture, or volume depletion. Diabetic ketoacidosis was more common with dapagliflozin than placebo (0.3% vs. 0.1%).
GLP-1 RA Trials
The LEADER (Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results) trial showed that liraglutide reduced the risk for major adverse cardiovascular events and death from cardiovascular causes (23). The FDA approved the use of liraglutide to reduce the risk for major cardiovascular events, including heart attack, stroke, and cardiovascular death, in adults with type 2 diabetes and ASCVD. Liraglutide also reduced the risk for new or worsening nephropathy, primarily as the result of a decrease in new-onset macroalbuminuria. In SUSTAIN (Trial to Evaluate Cardiovascular and Other Long-Term Outcomes With Semaglutide in Subjects With Type 2 Diabetes), semaglutide reduced the risk for both major adverse cardiovascular events and new or worsening nephropathy. The reduction in nephropathy risk was primarily the result of a decrease in new-onset macroalbuminuria (24).
This trial reported an increased incidence of retinopathy with semaglutide compared with placebo. The PIONEER (Peptide Innovation for Early Diabetes Treatment) trial compared oral semaglutide with placebo in a population mainly (85%) comprising patients with ASCVD or CKD. This trial found that oral semaglutide was noninferior to placebo for the primary composite outcome of major adverse cardiovascular events (25).
In EXSCEL (Exenatide Study of Cardiovascular Event Lowering), extended-release exenatide reduced the risk for major adverse cardiovascular events and all-cause mortality, although the latter finding was not statistically significant (26). Another trial that included participants with ASCVD or advanced (high) cardiovascular disease risk found that dulaglutide reduced the risk for major adverse cardiovascular events (26). These results were consistent across the subgroups of patients with and without established ASCVD. All-cause mortality did not differ between the 2 groups. This large outcomes trial was the first to show benefit in a high-risk primary prevention population (27).
Glucose-Lowering Therapies and Heart Failure
Thiazolidinediones should not be used in patients with symptomatic heart failure (28 –30). Metformin may be used in patients who have stable heart failure with adequate kidney function (31). The SAVOR-TIMI 53 (Saxagliptin Assessment of Vascular Outcomes Recorded in Patients With Diabetes Mellitus) study showed that patients treated with the DPP-4 inhibitor saxagliptin were more likely to be hospitalized for heart failure than those given placebo (3.5% vs. 2.8%, respectively) (32). Outcome trials of the DPP-4 inhibitors alogliptin, sitagliptin, and linagliptin have not demonstrated an increased risk for hospitalization for heart failure (33–35). No increased or decreased risk for heart failure hospitalization has been identified in the outcome trials of GLP-1 RAs (23, 24, 26, 27, 36).
Among patients with and those without a history of heart failure, SGLT2 inhibitors reduced the incidence of hospitalization for heart failure (37). Outcome trials of empagliflozin, canagliflozin, and dapagliflozin showed that these agents decreased the risk for heart failure hospitalization (19, 21, 22). Similar results were shown with canagliflozin in a population with diabetes and CKD (38).
INSULIN THERAPY
Many persons with type 2 diabetes ultimately require insulin therapy to achieve glycemic targets. Type 2 diabetes is a progressive condition; its progressive nature should be routinely discussed with patients. Providers should discuss the potential need for insulin to escalate therapy rather than presenting it as failure on the patient’s part. The functions and benefits of insulin use for achieving glycemic control as the disease progresses and other medications become less effective should be stressed to the patient. When initiating insulin therapy in type 2 diabetes, educating patients to selftitrate insulin doses on the basis of self-monitoring of blood glucose improves glycemic control (39). Patient education should also include diet, self-monitoring of blood glucose, and management of hypoglycemia in any patient using insulin.
Basal Insulin
The addition of basal insulin to metformin and other oral agents is the most convenient initial insulin therapy. Starting doses can be estimated on the basis of body weight (0.1 to 0.2 IU/kg per day) and the degree of hyperglycemia or may be given as a standard 10-IU daily dose. The dosage should be individually titrated every few days on the basis of self-monitored blood glucose levels. An evidence-based titration algorithm may be used. Patients may be instructed to self-titrate their basal insulin by setting a fasting glucose target and increasing their basal insulin by 2 IU every 3 days to reach their fasting plasma glucose target without hypoglycemia. If hypoglycemia occurs, the cause should be determined; if no clear remedial cause is found, the next dose should be lowered by 10% to 20%. Basal insulin limits hyperglycemia overnight and postprandially and restricts hepatic glucose production (40, 41). Long-acting insulin analogues or human neutral protamine Hagedorn (NPH) insulins are used to manage fasting glucose levels. Compared with NPH insulin, long-acting basal analogues (U-100 detemir or glargine) reduced the risk for hypoglycemia in clinical trials (42– 46), although this decrease may not persist over time (47). Newer, longer-acting basal analogues (degludec or U-300 glargine) have been shown to reduce hypoglycemia compared with U-100 glargine when used in combination with oral drug therapy (48 – 54). In clinical practice, these benefits may be modest compared with those of NPH (55).
Insulin costs have climbed steadily for more than 20 years, rapidly outpacing other medical expenses. These costs contribute to therapy nonadherence, because patients may ration or withhold insulin (56). Medication expense is a critical component of effective management and must be considered. Human insulin (regular and NPH) may be appropriate therapy for patients with type 2 diabetes who have a low risk for hypoglycemia, insulin resistance, less stringent HbA1c goals, or limited finances. Neutral protamine Hagedorn, 70/30 NPH/regular, and human regular insulin vials and pens are available for substantially less than the average wholesale price or National Average Drug Acquisition Cost at select pharmacies. Clinicians should be familiar with prescribing these insulins and with their use (55).
Prandial Insulin
Many patients with type 2 diabetes require pre-prandial insulin in addition to basal insulin to reach glucose targets. Dosing 4 IU or 10% of the amount of basal insulin before the largest meal or the meal with the greatest postprandial excursion is a safe method of initiating therapy. Preprandial insulin dosing may be intensified on the basis of patient needs. Patients with type 2 diabetes generally have more insulin resistance, require higher daily insulin doses (about 1 IU/kg), and have lower rates of hypoglycemia than patients with type 1 diabetes (57). Titration may be based on HbA1c levels or home glucose monitoring. As prandial insulin doses increase, particularly with the evening meal, providers should consider decreasing basal insulin doses to avoid hypoglycemia, particularly nocturnal hypoglycemia.
Concentrated Insulins
Several concentrated insulins are available for use by patients with type 2 diabetes. U-500 regular insulin is 5 times more concentrated than U-100 regular insulin. Regular U-500 insulin has characteristics similar to those of intermediate-acting (NPH) insulin and may be administered in 2 or 3 injections per day (58). U-200 degludec and U-300 glargine are 2 and 3 times more concentrated, respectively, than their U-100 formulations and may be useful in patients with higher basal insulin requirements. U-300 glargine is longer acting than U-100 glargine but has a slightly lower efficacy per unit injected (59, 60). A concentrated formulation of rapid-acting insulin lispro, U-200 (200 IU/mL), is also available. U-500 regular insulin is available in both vials and prefilled pens. A dedicated syringe for use with U-500 insulin is available. Other concentrated insulins are available only in prefilled pens to reduce potential errors in dosing.
Inhaled Insulin
Inhaled insulin is available for mealtime use, with a limited dosing range. Studies in persons with type 1 diabetes suggest more rapid pharmacokinetics compared with subcutaneous rapid-acting insulin (61). A pilot study found evidence that compared with injectable rapid-acting insulin, supplemental doses of inhaled insulin administered on the basis of postprandial glucose levels may improve glycemic control without additional weight gain or hypoglycemia (62). Patients require spirometry studies (FEV1) to identify potential lung disease before and after initiating inhaled insulin treatment. Inhaled insulin is contraindicated in patients with chronic lung diseases, such as chronic obstructive pulmonary disease and asthma. Inhaled insulin is not recommended for persons who currently smoke or recently stopped smoking.
Combination Injectable Therapy
Providers may consider combination injectable therapy for patients whose basal insulin has been titrated appropriately to target fasting blood glucose values but whose HbA1c levels remain above target, or for those whose basal insulin dose is greater than 0.5 IU/kg per day. Basal insulin combined with GLP-1 RA therapy may improve blood glucose levels with less hypoglycemia and weight gain relative to basal–bolus insulin routines (63– 65). Available dual-combination products containing basal insulin plus a GLP-1 RA include insulin degludec plus liraglutide and insulin glargine plus lixisenatide.
Intensifying insulin therapy may include the addition of prandial insulin doses to basal insulin. Adding a single dose of prandial insulin before the largest meal of the day is effective and easy, and if necessary, it can be advanced to a routine with several prandial doses (66). Also, 2 doses of premixed insulin per day may be used in place of basal insulin in patients who need additional prandial insulin coverage. Both approaches have advantages and disadvantages. Basal–prandial routines provide more flexibility because patients can eat meals on irregular schedules more easily. Conversely, premixed insulin at 2 doses per day is a convenient method of spreading insulin across the day. Human insulins, separately or as premixed 70/30 formulations, are less costly than insulin analogues. Figure 2 outlines these various options and provides recommendations for further intensification to help achieve glycemic targets. Metformin therapy should be continued, whereas DPP-4 inhibitors and sulfonylureas usually are withdrawn, when patients advance to combination injectable regimens. Concurrent use of an SGLT2 inhibitor or thiazolidinedione may help improve glycemic control and reduce insulin requirements. Dose titration is important after insulin therapy progresses to a basal–prandial regimen. Adjustments should be made on the basis of glucose levels provided by data from continuous or self-monitoring.
From St. Mark’s Hospital and St. Mark’s Diabetes Center, Salt Lake City, Utah (K.D., J.J.C.); Touro University California, College of Osteopathic Medicine, Vallejo, California (J.H.S.); Abington Family Medicine, Jenkintown, Pennsylvania (N.S.); and Skaggs School of Pharmacy and Pharmaceutical Sciences, University of Colorado Anschutz Medical Campus, Aurora,
Colorado (J.T.). Acknowledgment: The authors thank Sarah Bradley and Mindy Saraco, MHA, for their invaluable assistance in the reviewing and editing of this manuscript. The full Standards of Medical Care in Diabetes–2020 was developed by the ADA’s Professional Practice Committee: Joshua J. Neumiller, PharmD, CDCES, FADCES (Chair); George Bakris, MD; William T. Cefalu, MD; Jill Crandall, MD; David D’Alessio, MD; Jennifer Green, MD; Elbert Huang, MD, MPH; Kathryn Evans Kreider, DNP, APRN, FNP-BC, BC-ADM; Christine G. Lee, MD, MS; Nisa Maruthur, MD, MHS; Anne Peters, MD; Maria Jose Redondo, MD, PhD, MPH; Jane Reusch, MD; Emily Weatherup, MS, RDN, CDCES; Jennifer Wyckoff, MD; and Deborah Young-Hyman, PhD, CDCES. Disclosures: Disclosures can be viewed at www.acponline.org/authors/icmje/ConflictOfInterestForms.do?msNum=M20-2470. Corresponding Author: Kacie Doyle-Delgado, DNP, APRN, St. Mark’s Hospital and St. Mark’s Diabetes Center, Internal Medicine at St. Mark’s, 1160 East 3900 South, Suite 1200, Salt Lake City, UT 84124; e-mail, kaciedoyle@gmail.com. Current author addresses and author contributions are available at Annals.org.

Recent Comments