
Beverly Jordan is a partner at a family-medicine clinic in Enterprise, Alabama. Enterprise is situated in “wiregrass country”—a largely rural region, encompassing southeastern Alabama and parts of Georgia and Florida, named for the ubiquitous vegetation that takes root in its sandy soil. Her clinic is one of a few offering primary care in the area; like many independent medical practices across the U.S., it has been gutted by the coronavirus pandemic. Even though her practice received a lifeline from the federal government’s Paycheck Protection Program (P.P.P.), Jordan had to take a pay cut, reduce staff hours, and lay off two new physicians who were about to start work. “For the first time in my career, we’re really just planning short-term,” she told me recently. “We’ve never had this level of insecurity.”
For decades, health care was America’s indomitable industry. While employment in other sectors—retail, manufacturing, construction—rose and fell with the business cycle, clinics, hospitals, and medical practices steadily added jobs. But the pandemic has changed health care’s trajectory. Hospitals now find themselves in dire financial straits as they forgo revenue from elective procedures, and a surge in unemployment is shifting patients from private insurance plans to Medicaid, which is less remunerative for doctors. Some rural hospitals, whose financial footing was already tenuous, are facing the prospect of closure.
Among the most vulnerable parts of the nation’s health-care system are family-medicine, internal-medicine, pediatric, and obstetrics-and-gynecology clinics. With covid-19 precautions in place, in-person appointments have dropped precipitously. In May, a survey of primary-care doctors found that nearly a fifth had temporarily closed their practices, owing to the pandemic, and two in five had laid off or furloughed staff. Primary-care clinics are tasked with keeping people healthy, and decades of research have shown that the care they provide is associated with better outcomes and lower costs. As my colleague Dhruv Khullar has written, the health consequences of these clinics’ closures could be significant. Vaccination rates for children have already begun to fall; patients are missing screenings proven to save lives; prescriptions are going unfilled. Chronic conditions could worsen; life expectancies could drop.
Even before the pandemic, primary care was in crisis. Primary-care doctors were already among the most poorly compensated physicians in the country; for medical students burdened with debt, those smaller salaries lessened the specialty’s allure. Experts have long warned of a shortage of doctors providing foundational forms of outpatient care, especially in rural areas. Last year, the Kaiser Family Foundation estimated that more than fourteen thousand primary-care physicians were needed to eliminate existing shortages.
For this article, I spoke with more than twenty primary-care physicians, from New York City to rural Nebraska and suburban Colorado. They work in single-physician practices, in multi-specialty groups, or as part of hospital systems. Nearly all of them described dramatic declines in revenue. Many benefitted from the P.P.P.; without it, some of their clinics might not have survived. All of the physicians expressed concern about how they would navigate the uncertainty ahead. “This is taking us down,” Jacqueline Fincher, an internist and the president of the American College of Physicians, told me. “We’re not going to have a vaccine and herd immunity for probably a year—so, is this sustainable for a year? The reality is, it’s probably not, certainly not for most small practices.” If many of them go out of business, the consequences for Americans’ health could be profound and enduring. What’s at stake is not just a pattern of health outcomes but the shape of the health-care system as a whole. The way that patients interact with their doctors and the path that American health care takes in the future may be about to shift.
The challenges facing primary care are rooted in the structure of the American health-care system. This system wasn’t designed at any one moment; instead, it has accreted over time, with each new layer seeking to compensate for the deficiencies of what came before. One of the most consequential layers is fee-for-service payment, which was codified as part of the Social Security Amendments of 1965—the law that created Medicare and Medicaid. In a fee-for-service setup, the payer, usually a health insurer or government agency, pays the health-care provider a set fee for any given service. Break your arm, and your insurance company might pay one fee for an X-ray, another for a splint, and a third for a follow-up visit. Though conceptually simple, the system has obvious flaws. It encourages health-care providers to offer more services, in order to earn more revenue, without necessarily controlling for quality. If one surgeon’s hip-replacement operation is successful, with no complications, but a second’s is complicated by infection, leading to a series of follow-up visits, their fees are still the same; in fact, the second hospital may make more money. “In a fee-for-service payment system,” Atul Gawande has written, “we are actually penalized for making the effort to organize and deliver care with the best service, quality, and efficiency we can.”
To address this problem, government programs and insurers have come up with alternative payment schemes—but, at a fundamental, almost philosophical, level, many of them still operate on a fee-for-service principle. In the nineteen-eighties, Medicare changed its approach to inpatient hospitalizations so that a single global fee covered a particular admission; in this system, a hospital is reimbursed at one payment level for a broken leg, at another for pneumonia, and at a third for sepsis. More recently, the Medicare Access and chip Reauthorization Act of 2015 pushed Medicare reimbursements away from a pure fee-for-service model and toward others that pay based on the quality of health care provided. Still, for the most part, it’s the provision of services that indicates that care has happened. Ultimately, when physicians are paid, it’s the number of office visits, lab tests, and surgeries that matters.
The fee-for-service principle reverberates through the whole health-care system, but it has especially dire consequences for primary care, because it favors discrete medical episodes over ongoing and preventative treatment. Payers routinely reimburse health-care providers for specialized procedures at high rates, but primary-care visits—which might include chronic-disease management, routine vaccinations, or smoking and diet counselling—generate lower revenues. This imbalance is due, in large part, to the Relative Value Update Committee (R.U.C.), an extraordinarily powerful group of doctors that advises the federal government on reimbursement rates for physicians. The R.U.C. consists of thirty-one doctors convened by the American Medical Association; it’s structured such that each specialty has an equal say. On the R.U.C., urology, thoracic surgery, and head-and-neck surgery have, individually, about the same representation as all of pediatrics. The Centers for Medicare and Medicaid Services (C.M.S.), which has final authority to set payment rates for Medicare, has in many years accepted the R.U.C.’s recommendations nearly ninety per cent of the time.
Primary-care groups and health-care policy experts have long contended that the R.U.C.’s choices favor procedures over the counselling, education, and chronic-disease management that form the basis of primary care. Twenty years ago, Don Berwick, the co-founder of the Institute for Healthcare Improvement and a mentor of mine, called for a total reimagining of health-care reimbursement in a speech that has since become famous in industry circles. Addressing an audience at the institute’s annual meeting, Berwick told the story of a Montana forest fire, from 1949, that killed most members of a team of firefighters. When the firefighters finally realized the imminent danger posed by the blaze, they tried to outrun it—but they did so while shouldering heavy equipment, including their Pulaskis, special firefighting axes that combine an axe head with an adze. The firefighters did not recognize that, in this new scenario, their old tools no longer served them; many died carrying them.
The health-care system, Berwick said, was falling into the same trap: clinging to a sometimes burdensome tool, no matter the circumstances. “Our Pulaski,” he argued, “is the encounter—the visit.” A better health-care system could only be built if “scientists, professionals, patients, payers, and the health-care workforce” agreed “that the product we choose to make is not visits. Our product is healing relationships.” In 2010, President Barack Obama, in a recess appointment, made Berwick the acting administrator of C.M.S.; he resigned, in 2011, when he concluded that he would be unable to win confirmation from Republicans in the Senate.
Among other things, the structural bias in favor of procedures and office visits has prevented telemedicine—which could make outpatient care more affordable, accessible, and consistent—from gaining a foothold. For decades, Medicare only paid for telemedicine visits if a patient lived in a designated “rural” area or received the treatment in a medical setting; effectively, for many people, telemedicine had to take place in a doctor’s office. The pandemic has changed this equation. In March, the federal government expanded the list of telemedicine services eligible for Medicare reimbursement. Clinics across the country, seeing telemedicine as both a way to provide care and a financial lifeline, raced to embrace phone and video visits almost overnight. “I was so close to getting a ninety-year-old woman to turn on a video call,” Lalita Abhyankar, a family-medicine doctor in New York City, told me. Abhyankar persisted because she’s found that, on the whole, patients become enthusiastic about virtual visits after trying them. Doctors, for their part, have found value in the glimpses that such visits offer of their patients’ home lives. Early in the covid-19 crisis, when I began conducting telemedicine visits with my own patients, I was surprised to discover that the technology created a feeling of camaraderie. The power dynamic diminished; conversing from our respective apartments, we were on equal footing.
For all the promise of this ongoing telemedical experiment, the future of primary care as a whole remains unclear. C.M.S. has said that the current dispensation is only a temporary emergency accommodation; if support for telemedicine stops before the pandemic does, our country will be taking a big risk. One preview of what might happen comes from studies assessing health outcomes after a patient’s primary-care doctor retires. Such patients don’t face a society-wide diminution in access to primary care; in many cases, they can switch to another physician without undue difficulty. Even so, a recent review of these studies found that nearly all patients experienced unfavorable outcomes, among them difficulty renewing prescriptions and increased use of high-cost care.
Labor economists have long studied a phenomenon called hysteresis: in economics, it refers to a situation in which high unemployment caused by a particular event develops an inertia of its own, remaining elevated even after the initial cause has abated. Nobody is quite sure what causes hysteresis. Do workers’ skills erode? Or do firms find that they can get along with fewer workers? In any case, now that the pandemic has caused extended mass unemployment, hysteresis could play a major role in our society—and our health care. In theory, a physician can sit out the lean times and return to practice once patient volume rebounds; during the Great Depression, for instance, some small-town doctors made house calls and accepted barter payments until the crisis ended. But the situation today is different. A modern medical practice needs physical space, an electronic records system, malpractice insurance, and back-office support to handle the byzantine medical coding on which reimbursement depends. Hanging out a shingle in twenty-first-century America requires more than a diploma; it requires capital.
Patients may also respond in an enduring way to what seems to be a temporary disruption of the doctor-patient relationship. In ordinary times, engaging people in the treatment of chronic conditions can be a fraught endeavor: a patient who’s easily persuaded to take an antibiotic for a urinary-tract infection might nevertheless resist taking a medication aimed at preventing complications from high blood pressure down the road. Regular checkups help patients develop and maintain fragile habits that the pandemic may have disrupted. “I have a diabetic patient who finally came in and hadn’t taken insulin in six weeks,” Gary LeRoy, a family physician in Ohio and the president of the American Academy of Family Physicians, told me. “It’s, like, ‘Why the heck did you not call?’ But, then, I don’t like going to the dentist—and if my dentist says, ‘Well, we’re not doing visits now,’ I think, Yay! I don’t have to go to the dentist,” he said. “It gives you an excuse to not do the right thing for yourself.”
There are steps that governments and insurers could take now to prevent the crisis from worsening. Many commercial insurers and state-administered Medicaid programs still don’t reimburse video visits at the same rates as in-person care; parity is even less common for telephone visits, which are particularly useful for the elderly and for those in low-income or rural communities who don’t have access to high-speed Internet. Some surveys of primary-care practices show that more than half of them haven’t yet received reimbursement for most of their telemedicine visits in recent months—a significant problem at a time of financial strain.
Through the cares Act and subsequent legislation, Congress has allocated a hundred and seventy-five billion dollars for health-care expenses attributable to the pandemic. How that money will be spent, however, remains unclear; those funds are also supposed to cover aid for hospitals and covid-19 care for the uninsured, among other things, and a hundred and seventy-five billion sounds less impressive when set against the $3.6 trillion that America spent on health care in 2018. The P.P.P. has helped some primary-care practices, but this is only a temporary lifeline. Without either an increase in funding or a direct allocation aimed at primary care, it seems likely that many clinics will never receive the money they need to stave off closure.
Some policymakers and providers have proposed a more drastic response to the pandemic—one that’s long been contemplated by health-policy experts and is already getting a test drive as part of the Affordable Care Act. Instead of continuing to reimburse providers through a fee-for-service system, the federal government could shift payment for primary care and similar specialties to a so-called capitation model. Under this system, practices are reimbursed on a per-person, per-month basis, usually with some portion of the payment tied to quality measures, such as adjusted mortality and excess hospitalizations. Since the A.C.A.’s passage, C.M.S. has been shifting toward this payment model, using health-care networks called Accountable Care Organizations (A.C.O.s). (Texas’s U.T. Southwestern, Wisconsin’s ThedaCare, and New York and New Jersey’s Montefiore are examples of A.C.O.s.) Despite these efforts, most primary-care practices are still paid mainly on a fee-for-service basis.
“A crisis is a terrible thing to waste,” the economist Paul Romer once said. The weaknesses that have left our primary-care system so vulnerable to the pandemic have been understood for decades, yet change has come at a glacial pace; it’s been easy to ignore the system’s flaws because health-care spending has grown over time, with many health-care organizations prospering as a result. Why undertake dramatic change when there is always more money to go around? Before the 2008 financial crisis, Charles Prince, who was then the C.E.O. of Citigroup, was asked why his bank continued to participate in the speculative real-estate market, given concerns that the bubble would soon burst. “When the music stops, in terms of liquidity, things will be complicated,” he said. “But, as long as the music is playing, you’ve got to get up and dance.” For much of American health care, the music has stopped. The best way to address the emergency is by embracing a better system.
Clifford Marks is an emergency-medicine resident at the Icahn School of Medicine at Mount Sinai.
In 2020, the American Diabetes Association (ADA) made important additions to the section on pharmacologic approaches to glycemic treatment of type 2 diabetes in the Standards of Medical Care in Diabetes. On the basis of new evidence, the ADA added a recommendation on early combination therapy for type 2 diabetes to extend the time to treatment failure. It is now recommended that these drugs be considered for patients in whom atherosclerotic cardiovascular disease (ASCVD), heart failure, or chronic kidney disease (CKD) predominate. The full position statement on pharmacologic treatment can be accessed at care.diabetesjournals.org/content/43/Supplement_1/S98. This synopsis summarizes the recommendations related to pharmacologic management and highlights important evidence from recent large trials with cardiovascular and renal outcomes.
GUIDELINE DEVELOPMENT AND EVIDENCE GRADING
The Professional Practice Committee of the ADA is an expert committee that comprises physicians, diabetes educators, and others who have expertise in such areas as pediatric and adult endocrinology, epidemiology, public health, microvascular complications, cardiovascular risk management, preconception and pregnancy care, diabetes prevention and weight management, and the use of technology in diabetes. For the current revision, committee members systematically searched MEDLINE for pertinent studies published in English from 15 October 2018 to August–September 2019. Committee members reviewed selected studies and, on the basis of new evidence and as needed, revised recommendations, clarified previous recommendations, or aligned the strength of the wording to the evidence.
Recommendations are rated A (well-designed clinical trials or high-quality meta-analyses), B (well-conducted cohort studies), C (uncontrolled studies), or E (expert consensus or clinical experience). The ADA funds development of the Standards of Care from its general revenues, with no industry involvement or support. Detailed information about the committee members and their conflict-of-interest disclosures, methodology, and the complete Standards of Care can be downloaded at professional.diabetes.org/soc.
PHARMACOLOGIC THERAPY FOR TYPE 2
DIABETES: RECOMMENDATIONS
Metformin is the preferred initial pharmacologic agent for the treatment of type 2 diabetes (Grade A recommendation).
Early combination therapy can be considered in some patients at treatment initiation to extend the time to treatment failure (Grade A recommendation).
The early introduction of insulin should be considered if there is evidence of ongoing catabolism (weight loss), if symptoms of hyperglycemia are present, or when hemoglobin A1c (HbA1c) or blood glucose levels are very high (HbA1c >10% [86 mmol/mol], blood glucose ≥16.7mmol/L [300 mg/dL]) (Grade E recommendation).
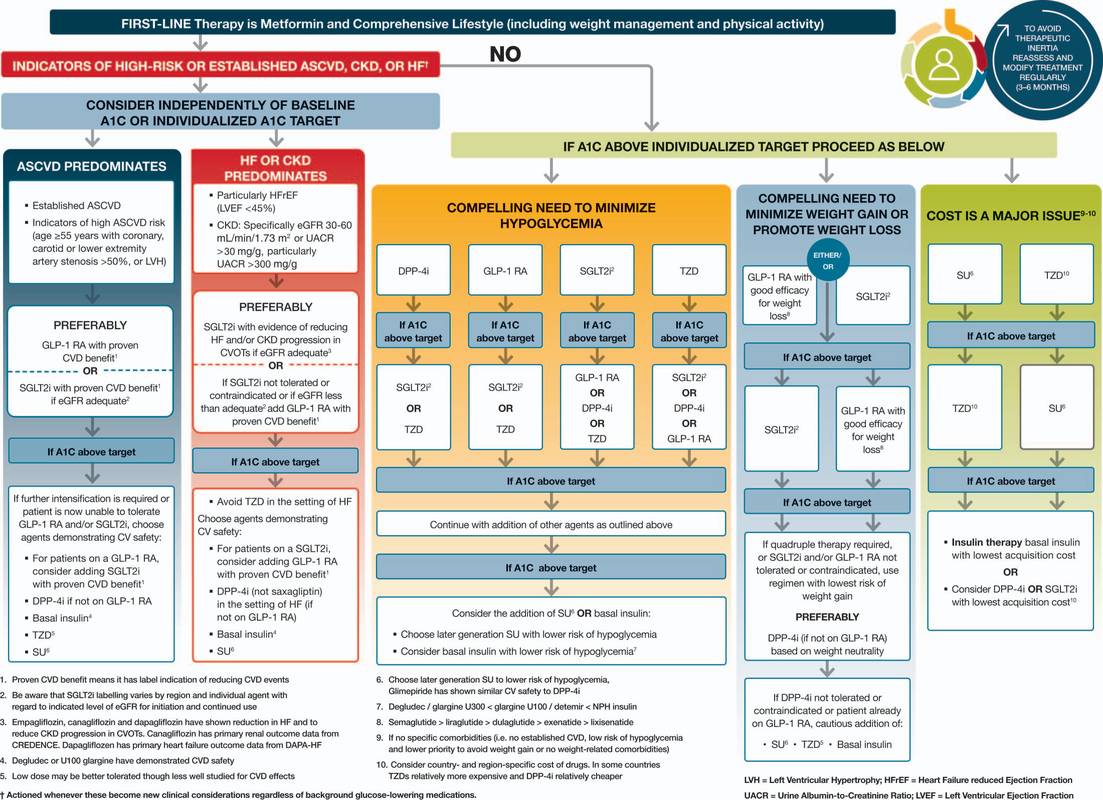
A patient-centered approach should be used to guide the choice of pharmacologic agents. Considerations include cardiovascular comorbid conditions, hypoglycemia risk, impact on weight, cost, risk for side effects, and patient preferences (Appendix Figure [available at Annals.org] and Figure 1) (Grade E recommendation).
Among patients with type 2 diabetes who have established ASCVD or indicators of high risk, established kidney disease, or heart failure, a sodium–glucose cotransporter-2 (SGLT2) inhibitor or glucagon-like peptide-1 receptoragonist (GLP-1 RA) with demonstrated cardiovascular disease benefit is recommended (Grade A recommendation).
In patients with type 2 diabetes who need greater glucose lowering than can be obtained with oral agents, GLP-1 RAs are preferred to insulin when possible (Grade B recommendation).
The medication regimen and medication-taking behavior should be reevaluated at regular intervals (every 3 to 6 months) and adjusted as needed to incorporate specific factors that affect choice of treatment (Grade E recommendation).
INITIAL THERAPY
The mainstay for initial treatment of type 2 diabetes includes therapeutic lifestyle change. In addition, metformin is recommended as the initial pharmacotherapyin most patients with type 2 diabetes at the time of diagnosis. Metformin is considered safe and effective (1% to 1.5% reduction in HbA1c levels) in patients with no contraindications (such as stage 4 or 5 CKD, advanced heart failure, or a history of lactic acidosis). It may reduce the risk for cardiovascular events and death in persons who are overweight or obese (1). In some patients, it causes substantial gastrointestinal side effects, including bloating, abdominal pain, and diarrhea. For those who do not tolerate the medication because of gastrointestinal side effects, the extended release formulation may be more acceptable. Long-term metformin use has been associated with vitamin B12 deficiency and worsening neuropathy (2). Periodic testing of vitamin B12 levels may be reasonable (3). The U.S. Food and Drug Administration (FDA) recommends that metformin be used only in patients with an estimated glomerular filtration rate of 30 mL/min/1.73 m2 or greater (4). For patients who do not tolerate metformin or have contraindications to its use, alternative pharmacotherapy should be considered.
COMBINATION THERAPY
For patients who have symptoms from advanced hyperglycemia, insulin therapy is recommended to reduce glucotoxicity and lipotoxicity. It is common practice to initiate insulin therapy for patients who presentwith the following: a blood glucose level of 16.7 mmol/L (300 mg/dL) or greater or an HbA1c concentration higher than 10% (86 mmol/mol), symptoms of hyperglycemia (namely polyuria or polydipsia), or evidence of catabolic weight loss or ketosis (Figure 2). As glucose toxicity resolves, simplifying the treatment regimen or transitioning to oral agents is often possible.
Type 2 diabetes is a progressive disease, and combination therapy is often needed to achieve or maintain glycemic targets (a comprehensive discussion on glycemic targets can be found at care.diabetesjournals.org/content/43/Supplement_1/S66). Current recommendations advise a stepwise approach to treatment for most patients, with the sequential addition of other medications to metformin therapy if the HbA1c target is not achieved after approximately 3 months. Initial combination therapy should be considered in patients presenting with HbA1c levels 1.5% to 2% above target, because most medications rarely decrease HbA1c concentrations by more than 1%. Data exist to support initial combination therapy (5, 6). This approach may be superior to sequential addition of medications for both achieving glycemic goals more rapidly and maintaining glycemic control for a longer period (7).
Second-line medication options include SGLT2 inhibitors, GLP-1 RAs, dipeptidyl peptidase-4 (DPP-4) inhibitors, thiazolidinedione, sulfonylureas, and basal insulin. Clinical evidence suggests that each new non-insulin medication added to metformin generally lowers HbA1c levels by approximately 0.7% to 1.0% (8, 9). The choice of agent to add to metformin therapy should be individualized on the basis of patient characteristics, preferences, and drug-specific effects. Important patient characteristics include ASCVD, risk for ASCVD, heart failure, CKD, other comorbid conditions, and the propensity for specific medication-related adverse effects. Medication considerations include efficacy, safety, tolerability, ease of use, and cost.
The first step in deciding which medication should be added to metformin is to determine whether the patient has established ASCVD or a high ASCVD risk (patients aged ≥55 years with coronary, carotid, or lower-extremity artery stenosis >50% or left ventricular hypertrophy), heart failure, or established CKD. If the patient has 1 of these characteristics, an SGLT2 inhibitor or GLP-1 RA with demonstrated CVD benefit is recommended. The addition of these medications should be considered independent from HbA1c level in this patient population. If a patient has heart failure or CKD, an SGLT2 inhibitor is recommended. If an SGLT2 inhibitor cannot be used, a GLP-1 RA should be administered. For patients without established ASCVD, indicators of high ASCVD risk, CKD, or heart failure, the choice of a second agent is based on avoidance of side effects, particularly hypoglycemia and weight gain; cost; and patient preferences (10). If the main patient factor is cost, a sulfonylurea or thiazolidinedione should be considered. These medications are inexpensive and potent. If the main concern is avoiding hypoglycemia, preferred medications include GLP-1 RAs, SGLT2 inhibitors, DPP-4 inhibitors, or a thiazolidinedione. If a compelling need exists to minimize weight gain or promote weight loss, the preferred pharmacotherapy should include GLP-1 RAs or SGLT2 inhibitors. Metformin and DPP-4 inhibitors tend to be weight neutral. Similar considerations apply to patients requiring a third agent to achieve glycemic goals. Treatment regimens should be reviewed continuously for side effects, efficacy, and treatment burden. Some patients may need their medication reduced or withdrawn. Common reasons include intolerable side effects, drug ineffectiveness, drug costs, or a change in glycemic targets. In older adults, relaxing glycemic targets and de-escalating therapy are often appropriate steps, depending on the patient’s health status.
Although many patients prefer oral medications, injectable agents often are needed to achieve treatment goals. The 2020 Standards of Care state that if injectable therapy is needed to reduce HbA1c levels, then a GLP-1 RA should be considered in most patients before the use of insulin. Most GLP-1 RAs are injected, although an oral formulation of semaglutide is now available (11). Meta-analyses comparing injectable GLP-1 RAs with insulin in patients needing further glucose lowering indicate similar efficacy between the 2 treatments (12–14). In addition, GLP-1 RAs have the benefit of causing weight loss, rather than weight gain, compared with insulin and carry a lower risk for hypoglycemia.
The cost of diabetes drugs has increased substantially during the past 2 decades (15). Diabetes drug prices may be a major source of stress for patients and contribute to reduced adherence (16). Cost-containing strategies may improve medication taking behaviors in some patients (17).

CARDIOVASCULAR AND RENAL OUTCOMES TRIALS
Because of concerns that diabetes drugs might lower glucose levels but lead to adverse cardiovascular outcomes, the FDA issued guidance for industry in 2008 requiring large long-term cardiovascular outcome trials of all new medications for treating type 2 diabetes (18). In such outcome trials of DPP-4 inhibitors, SGLT2 inhibitors, and GLP-1 RAs, the study drug is compared with placebo, with both agents given in addition to standard care.
DPP-4 Inhibitor Trials
Trials of DPP-4 inhibitors met the primary outcome of noninferiority, meaning the studies demonstrated that DPP-4 inhibitors do not increase adverse cardiovascular outcomes. However, DPP-4 inhibitors have not demonstrated superiority, meaning that they have not shown cardiovascular benefits relative to placebo.
SGLT2 Inhibitor Trials
EMPA-REG OUTCOME (Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients Removing Excess Glucose) showed that empagliflozin reduced the risk for major adverse cardiovascular events (a composite outcome of myocardial infarction, stroke, and cardiovascular death), cardiovascular death, and hospitalization for heart failure (19). These results led to an FDA indication for empagliflozin for reducing the risk for cardiovascular death in adults with type 2 diabetes and cardiovascular disease. A prespecified secondary analysis of the trial showed that empagliflozin also reduced the risk for incident or worsening nephropathy (20).
Canagliflozin reduced the risk for major adverse cardiovascular events but increased the risk for fracture and lower-limb amputation in CANVAS (Canagliflozin Cardiovascular Assessment Study) (21). The CREDENCE (Canagliflozin and Renal Events in Diabetes With Established Nephropathy Clinical Evaluation) trial involved patients with chronic diabetes-related kidney disease, most (99%) of whom were using an angiotensin-converting enzyme inhibitor or angiotensin-receptor blocker (21). In this trial, canagliflozin reduced the risk for worsening kidney disease and death (a composite outcome of end-stage kidney disease, doubling of serum creatinine levels, or death from renal or cardiovascular causes), major adverse cardiovascular events, and hospitalizations for heart failure. Canagliflozin did not statistically significantly increase the risk for lower-limb amputations, fractures, acute kidney in- jury, or hyperkalemia but did increase the risk for diabetic ketoacidosis (2.2 and 0.2 events per 1000 patient-years in the canagliflozin and placebo groups, respectively). In September 2019, the FDA approved canagliflozin to reduce the risk for end-stage kidney disease, doubling of serum creatinine levels, cardiovascular death, and hospitalization for heart failure in adults with type 2 diabetes and diabetic nephropathy with albuminuria greater than 300 mg/g.
In the DECLARE-TIMI 58 (Dapagliflozin Effect on Cardiovascular Events–Thrombolysis in Myocardial Infarction 58) trial, dapagliflozin met the prespecified criteria for noninferiority to placebo with regard to major adverse cardiovascular events, but superiority to placebo was not demonstrated (22). Dapagliflozin reduced the risk for a coprimary composite end point of cardiovascular death or hospitalization for heart failure, driven primarily by the hospitalization end point. No between-group differences were demonstrated for cardiovascular death, rate of amputation, fracture, or volume depletion. Diabetic ketoacidosis was more common with dapagliflozin than placebo (0.3% vs. 0.1%).
GLP-1 RA Trials
The LEADER (Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results) trial showed that liraglutide reduced the risk for major adverse cardiovascular events and death from cardiovascular causes (23). The FDA approved the use of liraglutide to reduce the risk for major cardiovascular events, including heart attack, stroke, and cardiovascular death, in adults with type 2 diabetes and ASCVD. Liraglutide also reduced the risk for new or worsening nephropathy, primarily as the result of a decrease in new-onset macroalbuminuria. In SUSTAIN (Trial to Evaluate Cardiovascular and Other Long-Term Outcomes With Semaglutide in Subjects With Type 2 Diabetes), semaglutide reduced the risk for both major adverse cardiovascular events and new or worsening nephropathy. The reduction in nephropathy risk was primarily the result of a decrease in new-onset macroalbuminuria (24).
This trial reported an increased incidence of retinopathy with semaglutide compared with placebo. The PIONEER (Peptide Innovation for Early Diabetes Treatment) trial compared oral semaglutide with placebo in a population mainly (85%) comprising patients with ASCVD or CKD. This trial found that oral semaglutide was noninferior to placebo for the primary composite outcome of major adverse cardiovascular events (25).
In EXSCEL (Exenatide Study of Cardiovascular Event Lowering), extended-release exenatide reduced the risk for major adverse cardiovascular events and all-cause mortality, although the latter finding was not statistically significant (26). Another trial that included participants with ASCVD or advanced (high) cardiovascular disease risk found that dulaglutide reduced the risk for major adverse cardiovascular events (26). These results were consistent across the subgroups of patients with and without established ASCVD. All-cause mortality did not differ between the 2 groups. This large outcomes trial was the first to show benefit in a high-risk primary prevention population (27).
Glucose-Lowering Therapies and Heart Failure
Thiazolidinediones should not be used in patients with symptomatic heart failure (28 –30). Metformin may be used in patients who have stable heart failure with adequate kidney function (31). The SAVOR-TIMI 53 (Saxagliptin Assessment of Vascular Outcomes Recorded in Patients With Diabetes Mellitus) study showed that patients treated with the DPP-4 inhibitor saxagliptin were more likely to be hospitalized for heart failure than those given placebo (3.5% vs. 2.8%, respectively) (32). Outcome trials of the DPP-4 inhibitors alogliptin, sitagliptin, and linagliptin have not demonstrated an increased risk for hospitalization for heart failure (33–35). No increased or decreased risk for heart failure hospitalization has been identified in the outcome trials of GLP-1 RAs (23, 24, 26, 27, 36).
Among patients with and those without a history of heart failure, SGLT2 inhibitors reduced the incidence of hospitalization for heart failure (37). Outcome trials of empagliflozin, canagliflozin, and dapagliflozin showed that these agents decreased the risk for heart failure hospitalization (19, 21, 22). Similar results were shown with canagliflozin in a population with diabetes and CKD (38).
INSULIN THERAPY
Many persons with type 2 diabetes ultimately require insulin therapy to achieve glycemic targets. Type 2 diabetes is a progressive condition; its progressive nature should be routinely discussed with patients. Providers should discuss the potential need for insulin to escalate therapy rather than presenting it as failure on the patient’s part. The functions and benefits of insulin use for achieving glycemic control as the disease progresses and other medications become less effective should be stressed to the patient. When initiating insulin therapy in type 2 diabetes, educating patients to selftitrate insulin doses on the basis of self-monitoring of blood glucose improves glycemic control (39). Patient education should also include diet, self-monitoring of blood glucose, and management of hypoglycemia in any patient using insulin.
Basal Insulin
The addition of basal insulin to metformin and other oral agents is the most convenient initial insulin therapy. Starting doses can be estimated on the basis of body weight (0.1 to 0.2 IU/kg per day) and the degree of hyperglycemia or may be given as a standard 10-IU daily dose. The dosage should be individually titrated every few days on the basis of self-monitored blood glucose levels. An evidence-based titration algorithm may be used. Patients may be instructed to self-titrate their basal insulin by setting a fasting glucose target and increasing their basal insulin by 2 IU every 3 days to reach their fasting plasma glucose target without hypoglycemia. If hypoglycemia occurs, the cause should be determined; if no clear remedial cause is found, the next dose should be lowered by 10% to 20%. Basal insulin limits hyperglycemia overnight and postprandially and restricts hepatic glucose production (40, 41). Long-acting insulin analogues or human neutral protamine Hagedorn (NPH) insulins are used to manage fasting glucose levels. Compared with NPH insulin, long-acting basal analogues (U-100 detemir or glargine) reduced the risk for hypoglycemia in clinical trials (42– 46), although this decrease may not persist over time (47). Newer, longer-acting basal analogues (degludec or U-300 glargine) have been shown to reduce hypoglycemia compared with U-100 glargine when used in combination with oral drug therapy (48 – 54). In clinical practice, these benefits may be modest compared with those of NPH (55).
Insulin costs have climbed steadily for more than 20 years, rapidly outpacing other medical expenses. These costs contribute to therapy nonadherence, because patients may ration or withhold insulin (56). Medication expense is a critical component of effective management and must be considered. Human insulin (regular and NPH) may be appropriate therapy for patients with type 2 diabetes who have a low risk for hypoglycemia, insulin resistance, less stringent HbA1c goals, or limited finances. Neutral protamine Hagedorn, 70/30 NPH/regular, and human regular insulin vials and pens are available for substantially less than the average wholesale price or National Average Drug Acquisition Cost at select pharmacies. Clinicians should be familiar with prescribing these insulins and with their use (55).
Prandial Insulin
Many patients with type 2 diabetes require pre-prandial insulin in addition to basal insulin to reach glucose targets. Dosing 4 IU or 10% of the amount of basal insulin before the largest meal or the meal with the greatest postprandial excursion is a safe method of initiating therapy. Preprandial insulin dosing may be intensified on the basis of patient needs. Patients with type 2 diabetes generally have more insulin resistance, require higher daily insulin doses (about 1 IU/kg), and have lower rates of hypoglycemia than patients with type 1 diabetes (57). Titration may be based on HbA1c levels or home glucose monitoring. As prandial insulin doses increase, particularly with the evening meal, providers should consider decreasing basal insulin doses to avoid hypoglycemia, particularly nocturnal hypoglycemia.
Concentrated Insulins
Several concentrated insulins are available for use by patients with type 2 diabetes. U-500 regular insulin is 5 times more concentrated than U-100 regular insulin. Regular U-500 insulin has characteristics similar to those of intermediate-acting (NPH) insulin and may be administered in 2 or 3 injections per day (58). U-200 degludec and U-300 glargine are 2 and 3 times more concentrated, respectively, than their U-100 formulations and may be useful in patients with higher basal insulin requirements. U-300 glargine is longer acting than U-100 glargine but has a slightly lower efficacy per unit injected (59, 60). A concentrated formulation of rapid-acting insulin lispro, U-200 (200 IU/mL), is also available. U-500 regular insulin is available in both vials and prefilled pens. A dedicated syringe for use with U-500 insulin is available. Other concentrated insulins are available only in prefilled pens to reduce potential errors in dosing.
Inhaled Insulin
Inhaled insulin is available for mealtime use, with a limited dosing range. Studies in persons with type 1 diabetes suggest more rapid pharmacokinetics compared with subcutaneous rapid-acting insulin (61). A pilot study found evidence that compared with injectable rapid-acting insulin, supplemental doses of inhaled insulin administered on the basis of postprandial glucose levels may improve glycemic control without additional weight gain or hypoglycemia (62). Patients require spirometry studies (FEV1) to identify potential lung disease before and after initiating inhaled insulin treatment. Inhaled insulin is contraindicated in patients with chronic lung diseases, such as chronic obstructive pulmonary disease and asthma. Inhaled insulin is not recommended for persons who currently smoke or recently stopped smoking.
Combination Injectable Therapy
Providers may consider combination injectable therapy for patients whose basal insulin has been titrated appropriately to target fasting blood glucose values but whose HbA1c levels remain above target, or for those whose basal insulin dose is greater than 0.5 IU/kg per day. Basal insulin combined with GLP-1 RA therapy may improve blood glucose levels with less hypoglycemia and weight gain relative to basal–bolus insulin routines (63– 65). Available dual-combination products containing basal insulin plus a GLP-1 RA include insulin degludec plus liraglutide and insulin glargine plus lixisenatide.
Intensifying insulin therapy may include the addition of prandial insulin doses to basal insulin. Adding a single dose of prandial insulin before the largest meal of the day is effective and easy, and if necessary, it can be advanced to a routine with several prandial doses (66). Also, 2 doses of premixed insulin per day may be used in place of basal insulin in patients who need additional prandial insulin coverage. Both approaches have advantages and disadvantages. Basal–prandial routines provide more flexibility because patients can eat meals on irregular schedules more easily. Conversely, premixed insulin at 2 doses per day is a convenient method of spreading insulin across the day. Human insulins, separately or as premixed 70/30 formulations, are less costly than insulin analogues. Figure 2 outlines these various options and provides recommendations for further intensification to help achieve glycemic targets. Metformin therapy should be continued, whereas DPP-4 inhibitors and sulfonylureas usually are withdrawn, when patients advance to combination injectable regimens. Concurrent use of an SGLT2 inhibitor or thiazolidinedione may help improve glycemic control and reduce insulin requirements. Dose titration is important after insulin therapy progresses to a basal–prandial regimen. Adjustments should be made on the basis of glucose levels provided by data from continuous or self-monitoring.
From St. Mark’s Hospital and St. Mark’s Diabetes Center, Salt Lake City, Utah (K.D., J.J.C.); Touro University California, College of Osteopathic Medicine, Vallejo, California (J.H.S.); Abington Family Medicine, Jenkintown, Pennsylvania (N.S.); and Skaggs School of Pharmacy and Pharmaceutical Sciences, University of Colorado Anschutz Medical Campus, Aurora,
Colorado (J.T.). Acknowledgment: The authors thank Sarah Bradley and Mindy Saraco, MHA, for their invaluable assistance in the reviewing and editing of this manuscript. The full Standards of Medical Care in Diabetes–2020 was developed by the ADA’s Professional Practice Committee: Joshua J. Neumiller, PharmD, CDCES, FADCES (Chair); George Bakris, MD; William T. Cefalu, MD; Jill Crandall, MD; David D’Alessio, MD; Jennifer Green, MD; Elbert Huang, MD, MPH; Kathryn Evans Kreider, DNP, APRN, FNP-BC, BC-ADM; Christine G. Lee, MD, MS; Nisa Maruthur, MD, MHS; Anne Peters, MD; Maria Jose Redondo, MD, PhD, MPH; Jane Reusch, MD; Emily Weatherup, MS, RDN, CDCES; Jennifer Wyckoff, MD; and Deborah Young-Hyman, PhD, CDCES. Disclosures: Disclosures can be viewed at www.acponline.org/authors/icmje/ConflictOfInterestForms.do?msNum=M20-2470. Corresponding Author: Kacie Doyle-Delgado, DNP, APRN, St. Mark’s Hospital and St. Mark’s Diabetes Center, Internal Medicine at St. Mark’s, 1160 East 3900 South, Suite 1200, Salt Lake City, UT 84124; e-mail, kaciedoyle@gmail.com. Current author addresses and author contributions are available at Annals.org.

Recent Comments