
Organizational efforts to improve health care professionals’ well-being should be guided by acarefully crafted strategy supported by appropriate tactics. Many organizations mistake aconceptual model or a collection of tactics for a strategy. Strategies should relate to enduringthematic approaches that will be pursued to make progress toward long-term goals, whereastactics refer to specific initiatives or programs intended to advance a component of thestrategy. Only after a strategy is developed can the optimal tactics to drive progress bedetermined and prioritized. A strategy to promote well-being must be tailored to meet theunique challenges, opportunities, and goals of each organization. Although customization is necessary, we believe several fundamental components can provide a blueprint for the well-being strategy of most health care organizations. The authors propose four such components:foundational programs, cultural transformation, rapid iterative experimentation, andsustainability. They also offer select insights on defining tactics and strategies.
The epidemic of occupational burnout among clinicians and its effects on quality of care, health carecosts, access, and patient experience are now widely recognized.1 Perhaps more important, we alsorecognize the fact that this challenge is driven by problems in the work environment and the healthcare delivery system. Vanguard organizations have committed themselves to address this issue and have initiated robust efforts to reduce occupational distress and cultivate clinician well-being.
The Importance of Strategy
To be effective, organizational efforts to improve well-being require a carefully crafted strategy supported by appropriate tactics. Unfortunately, many organizations mistake a conceptual model ora collection of tactics for a strategy. Articles have recently been published on design considerationsfor organizational programs on well-being; the role, responsibilities, and performance metrics for Chief Wellness Officers (CWOs); how to engage hospital boards; the importance of organizational culture in these efforts; and the roles and responsibilities of executive leaders. In this perspective, we share our approach for the development of an organizational strategy to promotewell-being.
Many physicians and health care professionals lack sophistication on what it means to develop a strategic plan and often confuse tactics for strategy. Strategies should relate to enduring thematic approaches that will be pursued to make progress toward the long-term goals (Figure 1). In contrast, tactics refer to specific initiatives or programs intended to advance a component of the strategy.

A strategy to promote health care professional well-being is most effective when designed to meet the unique challenges, opportunities, and goals of each organization. The size and geographic distribution of the enterprise, the scope of the mission/charge, and the resources available all influence the strategy. Although customization is necessary, we believe that several fundamental components can provide a blueprint for the well-being strategy of most organizations. In this perspective, we propose four such components: foundational programs, cultural transformation, rapid iterative experimentation, and sustainability.
Foundational Programs
We use the term “foundational programs” to encompass effective, evidence-based interventions for which best practices exist. Foundational programs that should be implemented across all healthcare institutions to facilitate well-being include:
- Safety-net resources for clinicians in distress10,11
- Resources to address the needs of individuals during major life transitions12-16
- An appropriate array of evidence-based self-care and wellness promotion offerings17
- Deliberate programs to promote collegiality and community at work18-21
- Assessment of well-being and its driver dimensions at recurring intervals coupled with a robust approach to disseminate results to clinical and operational leaders22,23
- Systemwide approaches that provide clinicians the opportunity to identify and prioritize the local factors that irritate them (“pebbles in the shoe”) and a process that empowers them to address these4,24,25
Specific considerations for such foundational programs are provided in Table 1.

Cultural Transformation
The second component of organizational strategy to promote well-being involves deliberate approaches to assess and strengthen key aspects of organizational culture.6,26,27 The principal goals of this effort are to:
- Incorporate consideration of the well-being of health care professionals into all operational decisions; and
- Imbue all leaders with the understanding that advancing the well-being of the people they lead is one of their principal responsibilities.
Cultural change in relevant dimensions that influence clinician well-being can be advanced by catalyzing a change in the organizational conversation, building coalitions, attending to leadership behaviors that promote professional fulfillment, advancing a mindset of distributed ownership of health care professional well-being, creating a network of change agents in each work unit (department, division, section, and clinic), and creating visibility and accountability for well-being performance metrics (department and work-unit leaders, executives, and board) (Figure 2).6

Culture refers to the shared beliefs, values, and social practices of a group. Where shared beliefs and values are contrary to practices, discovery conversations can till fertile ground for organizational development. To some extent, organizations and their culture can be considered the ongoing conversation that shapes the patterns of both thinking and relating that exist among the members of an organization.26 Frequently, this organizational conversation becomes ossified. Deliberate efforts to alter a fixed organizational conversation can be one approach to promoting cultural change.26 A variety of intentional approaches to catalyze a new organizational conversation through communication strategies, appreciative inquiry, focus groups or town halls, and other tactics can help infuse clinician well-being into the organizational culture. A correctly placed executive leader with sufficient authority and resources to drive change, such as a CWO, can help advance such organizational efforts. Deliberate thought on how to construct, sequence, augment, learn from, and follow-up on conversations can be an important component of the cultural change strategy to advance clinician well-being within the organization.
Efforts to build a coalition to advance well-being should begin with the CWO engaging other key leaders whose work has a direct link to clinician well-being. This includes the Chief Quality Officer, Chief Medical Officer, Chief Experience Officer, Chief Medical Information Officer, Dean of Faculty Development, Chief HR Officer, Chief Diversity Officer, and the relevant operational leaders. Typically, each of the leaders listed already oversees specific ongoing projects in which a greater emphasis on a well-being–related dimension might actually advance their projects while also improving clinician well-being. In other scenarios, these leaders may hold the keys to experimenting with alternatives to long-standing practices that undermine well-being goals. Such experiments are made possible through deliberate conversations to achieve cultural alignment.
Attention to leadership behaviors includes increased organizational focus on leadership selection, development, and feedback. We recommend annual assessment of leadership performance by the clinicians under each leader’s supervision along with confidential feedback to the leader.7 This feedback should be accompanied by opportunities for coaching, mentorship, and professional development to advance the leader’s skills in relevant areas.28 Among the myriad skills leaders must develop, those most critical to fostering the well-being of those they lead include keeping people informed, seeking their input in decision-making, understanding their personal passions, facilitating career development, and recognizing accomplishments. Incentives for achieving improvement targets related to clinician well-being can also be incorporated into the compensation structure for each leader and advance the mindset of distributed ownership throughout the organization.
Creating relevant metrics and goals for executive leaders with accountability to the hospital or organization’s board can establish well-being as a priority across all levels of leadership, foster transparency, and cultivate a mindset of distributed ownership. In addition to measures of professional fulfillment and occupational distress (burnout), these metrics may include leading indicators or directional measures such as the amount of time clinicians spend on documentation after hours, the efficiency of the procedural practice environment (e.g., operating room turnaround times), and assessments of teamwork. There are multiple assessment instruments measuring domains relevant to well-being (e.g., burnout, professional fulfillment, fatigue, work–life integration, and overall well-being). Ideally, organizations should select standardized instruments shown to correlate to the outcomes of interest (e.g., safety, quality, productivity, and turnover) and for which national benchmarks are available to provide context.
Creating a network of change agents within each work unit can also help advance well-being at the local level. Organizations have been successful using both formal appointments and titles, such as Department Well-being Director (the title used by Stanford Medicine), or with less formal appointments designated by some organizations as Wellness Champions. We believe a formal appointment along with a modest amount of protected time to execute the role increases impact and effectiveness. These individuals should be selected by the leader of the department or work unit. Their primary qualifications are their ability to work with that leader, the respect of their team members, and their commitment to advancing well-being. These qualities are more important than expertise in well-being improvement science, which can be transmitted through training, development, and support of these change agents. Once in place and initial training is complete, these individuals can be a powerful conduit for disseminating interventions, driving local change, and providing bidirectional communication (i.e., disseminating what the organization is doing in relation to well-being and providing feedback on opportunities for improvement).
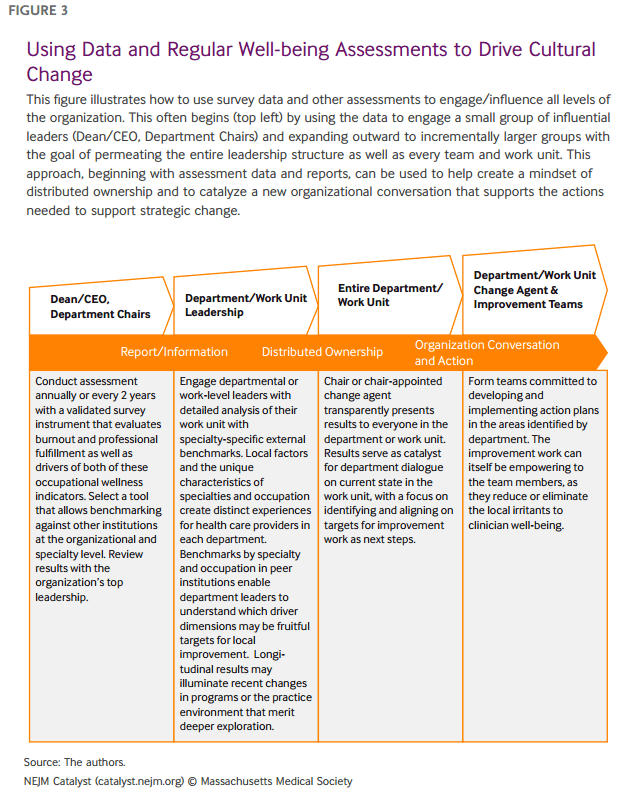
The regular assessment of well-being provides value beyond generating a snapshot of an organization’s current state. It can also be a tool for engaging leaders within the organization, broadening the sense of ownership of health care professional well-being, stimulating discussions that illuminate the perspectives of health care professionals, and mobilizing improvement efforts that focus on local and organizational needs. Hence, the assessment can become a powerful catalyst for cultural transformation (Figure 3).
Rapid Iterative Experimentation
The third component of organizational strategy to promote well-being involves rapid iterative experimentation, which is needed when a driver dimension (in this case, one that contributes to burnout or professional fulfillment) has been identified but for which effective tactics to improve that driver are not yet established (i.e., there is not yet an evidence-based foundational program). Rather than design a program and pursue widespread implementation, organizations should pursue an iterative experimental approach that first pilots novel programs, rigorously evaluates their efficacy, refines or replaces the intervention on the basis of results, and only scales programs after they have been both proven effective and optimized. The duration of the evaluation interval for this process must be tailored to the nature of the intervention but typically may range from 6 to 18 months (Figure 4).

This framework is analogous to the translational science approach to improving care for patients with a given disease. Investigators must first pursue basic discovery research that identifies key disease mechanisms. Once identified, it is often necessary to develop a new agent to target that disease pathway. Once developed, the agent must be rigorously tested, initially in the laboratory and subsequently in the clinic, to determine whether it hits the intended target and ultimately improves the patient’s clinical outcome. It is typical that multiple attempts must be made before an effective approach is identified. If the initial effort to modify a critical disease pathway is ineffective, the investigators do not abandon trying to target that pathway but instead develop derivative or alternative agents to try to hit the target more effectively. Only after the approach is proven to be effective is it broadly scaled.
It should be noted that, as in other areas of medical science, not all sites or investigators will engage in basic discovery work. Most, however, will need to develop (or adapt) interventions specific to the needs of their organization, evaluate their effectiveness, and optimize the interventions before they are broadly scaled. Once effective interventions have been scaled at one organization as well as adopted and proven effective by other organizations, they become best practices and may be considered as foundational programs by other organizations.
A number of the drivers affecting clinician well-being have been identified, including: excessive workload, inefficiencies in the practice environment, inadequate flexibility/control over work, issues with work–life integration, problems with teamwork, deficits in self-valuation, individual–organizational values misalignment, and the need for more effective first-line leaders. For several critical drivers of professional fulfillment and burnout, the optimal interventions to facilitate improvement are poorly defined. Our approach enables organizations to invest their limited resources wisely by developing and piloting tactical approaches and optimizing them first rather than wasting resources scaling well-intended but ineffective approaches.
One example of an intervention targeting a key well-being driver dimension that has successfully progressed through this continuum is tactical use of structured discussion through commensality groups to reduce isolation, cultivate collegiality, and enhance meaning in work. After discovery research identified isolation and erosion of collegiality as a driver of burnout in physicians, an initial intervention was designed to enhance community and meaning in work. The intervention was subsequently tested in a randomized trial and proved to be effective.19 However, logistical considerations, complexity, and cost were barriers to the scalability. Accordingly, rather than scale that intervention, a derivative approach that was more feasible to disseminate was tested. When the derivative approach also proved effective,18 it was scaled across the organization and subsequently across other organizations. It has now graduated to the foundational programs category.
Sustainability
A final key component of organizational strategies to promote well-being is sustainability. Organizational programs to improve well-being are typically small in relation to the size and complexity of the organizations in which they function and the magnitude of the challenge they are commissioned to address. The needs are great, the challenges numerous, and the potential opportunities for intervention myriad. There is also typically diversity of opinion regarding which interventions are most important to pursue.
Sustainability involves assessing the resources available with respect to personnel, time, authority, influence, and financial resources and determining how to optimally deploy these when designing and evaluating tactical programs. As part of this, the CWO and well-being leaders must also consider whether their team’s primary role will be to design, own, or influence specific projects and initiatives. There are critical tactics for which it will be important for the team to own the spectrum from design through implementation. For others, they may maximize their impact on well-being by designing and piloting an initiative but handing it off to other groups for broad implementation. Expanded impact can also be achieved by influencing the structure and format of initiatives that will be owned and implemented by others. A small team can have an outsized impact on the organization if they have a clear understanding of their strategy, recognize the key tactics they have prioritized, and magnify their impact through advocacy and influence rather than trying to own and implement every initiative.
Finally, efforts to advance the well-being of clinicians also require an operational infrastructure for people management, budget oversight, event planning, project management, communications, scheduling, and administrative support. Programs that fail to appropriately account for these needs are at high risk of becoming overextended, taking on too much too fast, and failing in execution. Overtly incorporating sustainability into the core strategic plan acknowledges these aspects, helps the team identify and execute on prioritized initiatives, and drives sustained progress (Table 2).


Effective Planning and Attention to Process
Organizational efforts to improve well-being require a long-term strategy, careful planning, and meticulous execution.
We have detailed four core components — foundational programs, cultural transformation, rapid iterative experimentation, and sustainability — that constitute a blueprint for organizations to address their unique challenges, opportunities, and goals as they design their well-being strategy. It is only after such an organization-specific strategy is developed from this framework that the specific tactics to drive progress can be determined and prioritized. The tactics selected will vary from one organization to another in accord with the organization-specific strategy. The strategy represents the longer-term plan to drive organizational progress and should undergo minimal changes year to year, even though the tactics and programs will evolve over time as their effectiveness is assessed, new approaches are identified, and overall progress is assessed.
Tait Shanafelt, MD
Professor of Medicine, Chief Wellness Officer, and Associate Dean, Stanford University School of
Medicine, Stanford, California, USA
Sherilyn Stolz
Executive Administrative Director, Stanford Medicine WellMD Center, Stanford University School
of Medicine, Stanford, California, USA
Jill Springer
Administrative Director, Stanford Medicine WellMD Center, Stanford University School of
Medicine, Stanford, California, USA
Daniel Murphy, MD
Professor of Pediatrics, Stanford University School of Medicine, Stanford, California, USA
Bryan Bohman, MD
Clinical Professor, Anesthesiology, Perioperative and Pain Medicine, Stanford Medicine, Stanford,
California, USA
Mickey Trockel, MD, PhD
Associate Professor, Psychiatry and Behavioral Sciences, Stanford University School of Medicine,
Stanford, California, USA
Disclosures: Funding for this study was provided by Stanford Medicine WellMD Center. Tait Shanafelt is coinventor of the Participatory Management Leadership Index and the Well-being Index instruments (Mayo Clinic holds the copyright for these instruments and has licensed them for use outside of Mayo Clinic, and Dr. Shanafelt receives a portion of any royalties paid to Mayo Clinic); he frequently gives grand rounds/keynote lecture presentations and provides advising for health care organizations, and he receives honoraria for some of these activities. Sherilyn Stolz, Jill Springer, Daniel Murphy, Bryan Bohman, and Mickey Trockel have nothing to disclose.
Recent Comments